This is my next entry to post for the MOWer’s blog. The subject is Symptoms. Wow! What a topic!

If you get symptoms of a cold, you see your internist, primary or family doctor. Symptoms of a cold are pretty simple and well-known: stuffy, runny nose, scratchy throat, post-nasal drip, etc. It’s interesting, but if you tell someone you have a cold, they know what symptoms you have already, and there are the traditional treatments as well. You can take a decongestant, drink tea with honey and lemon, take Tylenol if you run a fever or if you have a sore throat even. For all of us with spondyloarthropathies, symptoms can be as different from each other as night and day, as hard to notice from one person to the next, and often stump doctors, even those that specialize in our rare problems~the rheumatologists.
I have been dealing with what I thought at some points in time were unrelated symptoms, then at other times began to swear up and down that everything I have been through in all my years have been related to the spondyloarthropathies that I (will) have been diagnosed with finally! The most difficult issue with all of this is that when you go to the doctor with 1 or 2 symptoms at a time, the frustration will blow your mind. It isn’t cut and dry. There is no certainty that your doctor will give you a diagnosis or even treat you for that matter. Meanwhile, you are trapped in a world of pain, weakness, disability, loss of your old self, and a feeling that you could even be losing your mind! One thing is for sure, no matter what symptoms you end up with if you are lucky enough to have one or more spondyloarthropathy, the physical symptoms will be there, and they might be similar to those you meet in the same situation, but you may also notice that they all end up questioning their mental state! Yes, it’s true!

When you have certain physical symptoms and no lab tests or x-rays or similar tests to back them up, doctors begin to question automatically if you really have these physical symptoms or if they are manifestations of something else going on~depression, anxiety, a psychiatric condition, or perhaps you appear to have drug-seeking behaviors because you are showing no real signs of pain but wanting something for pain! Well, with all of this, it is only natural to begin questioning yourself, “Am I really feeling these symptoms? Is my neck really this stiff? Is my lower back hurting so bad, I cannot sleep at night? Are the bottoms of my feet so painful that if feels like I am walking on hot coals? Are my joints really so stiff and sore that I can’t move them for 2 hours after I awaken in the morning?” When we can’t really answer yes or no definitively, it gets pretty scary for us!!!

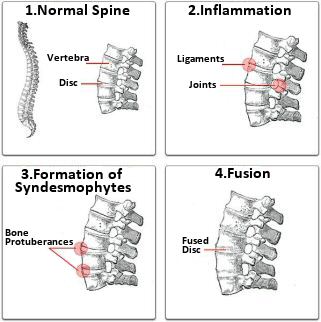
The symptoms are real, don’t get me wrong, and I am in no way trying to make them seem unreal or to make light of spondyloarthropathies or their symptoms. After all, I am a person with spondyloarthropothies, and I know how real they are and that the symptoms are definitely REAL!! So now let me just talk to you a little bit about what I had to go through to finally get someone, anyone, to listen to me about my symptoms. Spondyloarthropathies tend to attack the body’s major joints, primarily were ligaments attach to bone. Like myself, many who suffer from a spondyloarthropathy condition are likely to experience pain and reduced mobility in the ankles, knees, hips and lower back that is much more significant in the morning or when waking. These symptoms may become less severe as the day progresses and have often been much less severe following exercise. Patients, like myself, suffering from spondyloarthropathy may also experience pain or stiffness in the shoulders and wrists that follows the same progressive improvement in severity as the other joint pain. Patients may also experience pleuritic chest pain which is characterized by pain in the chest area that may or may not be accompanied with breathing difficulty. It also can be due to costochondritis, which I have often and is very, very painful!!! This symptom alone is not enough to diagnose a spondyloarthropathy as this form of chest pain is also a common symptom of pneumonia, viral illness, a pulmonary embolism, heart attack, lung cancer or a pleural tumor. For that reason, any chest pain should be considered serious and warrants a doctor’s immediate attention for further testing to rule out anything that is critical and must be addressed immediately.

Weight loss, fever and fatigue are also common symptoms that present with all of the spondyloarthropathy conditions. I would say that for me, in the earlier stages, weight loss was severe. Then I began to gain weight as the disease progressed. Fever and fatigue has been around for as long as I can remember. I have daily fevers, low-grade, in the late afternoon and during the night. Fatigue continues to be a problem for me. Although medications have helped, I still continue to get exhausted and tire easily. I have very little energy, and I also do not sleep well which only makes the problem worse. Some spondyloarthropathies may also cause what is commonly known as sausage digit–a swelling of the fingers or toes. I had the sausage digits on a couple of my toes, which finally went away after starting on a biologic–Remicade. Some patients will also suffer from a heart murmur that will need to be monitored by a doctor as well. I have a history of a heart murmur that comes and goes.

Rheumatoid arthritis is likely the medical condition most commonly confused with spondyloarthropathy but is generally able to be ruled out by tests that reveal the rheumatoid factor is not present in the patient’s blood. Of course, this is not always the case because even those people with RA do not always test positive for the rheumatoid factor. Also, since it is quite possible that spondyloarthropathies run in families, a patient’s family history is also a good indicator of whether or not their condition is a spondyloarthropathy or rheumatoid arthritis. Again, this is not always true either because many of us have no one in our families with a spondyloarthropathy. We do not know, however, if this is the case because there truly is no one in our family history with a spondyloarthropathy or if there is a family history, and perhaps no one ever did anything about it~diagnosis, treatment, etc.

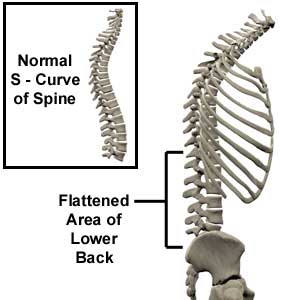
Initially, a patient suffering from spondyloarthropathy will experience pain or stiffness in the lower back; especially in the morning. That pain or stiffness will often gradually feel better throughout the day or following a period of exercise. Fatigue is also a common indicator that someone is suffering from this condition. They may feel worn out more quickly than previously or may feel tired much more often. In time the pain and stiffness in the lower back will spread further into the lower back and the buttocks. Treatment will likely not eliminate the symptoms entirely but should allow relief and prevent the condition from progressing further as quickly. Nothing has been proven to stop the progression of the condition entirely, but treatment will at least slow down the process. For many women, the first symptom is pain and stiffness in the neck, before the lower back, which does not mean that the lower back isn’t experiencing any problems. Many times, by the time, they feel symptoms in the lower back, the damage is already severe.


Because a major component of the eye is collagen just like the ligaments, tendons and tissue within joint spaces, it is reasonable to think that the eye would also be affected by the symptoms of spondylitis just like the joints. Thirty percent of people with spondylitis have had or will develop a potentially serious inflammation of the eye called iritis. (Acute anterior uveitis and iridocyclitis are additional medical terms to describe iritis.) I have had iritis/uveitis four times. Three of the four times I knew what to look for, but the first time, I didn’t even know that the inflammation was occurring. I was at my ophthalmologist for my yearly check up when it was found. This condition can cause blindness if not treated properly, so it is essential for you to recognize its signs and symptoms , and understand the important role you play in your eye health care. Symptoms often occur in one eye at a time, and they may include redness, pain, sensitivity to light, and skewed vision. By using a slit-lamp microscope, an ophthalmologist or specially trained optometrist can distinguish iritis from other causes of eye redness (such as from an allergy, trauma, or viral infection).[http://www.spondylitis.org/members/03.aspx?PgSrch=symptoms]

In a minority of individuals, the pain does not start in the lower back, but in a peripheral joint such as the hip, ankle, elbow, knee, heel or shoulder. This pain is commonly caused by enthesitis, which is the inflammation of the site where a ligament or tendon attaches to bone. Inflammation and pain in peripheral joints is more common in juveniles with ankylosing spondylitis (AS). This can be confusing since, without the immediate presence of back pain, AS may look like some other form of arthritis. Many people with AS also experience bowel inflammation, which may be associated with Crohn’s Disease or ulcerative colitis. Advanced symptoms can be chronic, severe pain and stiffness in the back, spine and possibly peripheral joints, as well as lack of spinal mobility because of chronic inflammation and possible spinal fusion. [http://www.spondylitis.org/about/as_sym.aspx]

I have had symptoms of inflammatory back/pelvis pain, unilateral or alternating buttock pain, enethesitis–inflammation where a tendon or ligament attaches to the bone, peripheral arthritis, arthritis of the small joints, heel pain, fatigue, the scaly patches on the skin caused by psoriasis, skin rashes that commonly appear as thickened red or brown spots, scaling rashes on the palms of the hands or soles of the feet, pain and swelling in the fingers or toes, sometimes the swelling causing a “sausage” appearance, small indentations, lifting and /or discoloration of the fingernails or toenails, fingernails and toenails which may become thickened and crumble as if infected by fungus, pain and swelling in the joints, pain and stiffness of the spine, especially after prolonged inactivity, fever and chills, cystitis, which is an inflammation of the bladder or urinary tract, causing frequent urination and a burning sensation when urinating, mouth ulcers, inflammatory eye conditions of the eye such as iritis/uveitis or conjunctivitis which can cause redness, pain, blurred vision and sensitivity to light. I was told that I have sacroiliac joint involvement. I was also told several years ago that where the spine meets the pelvis looks like it was crushed in an automobile accident when I had an MRI done. I never had my pelvis/SI joints crushed in an auto accident.

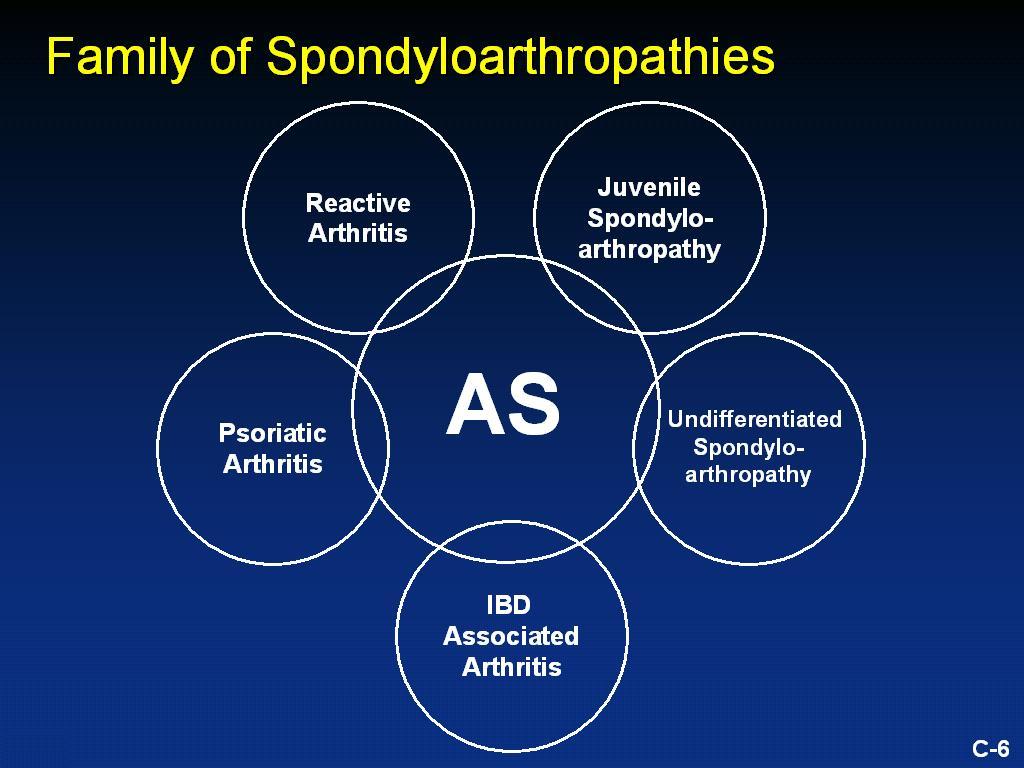
There are several types of spondyloarthropathies, and a big difference is age of onset and which sex it affects more. General onset of AS commonly occurs in younger people, between the ages of 17-45. However, it can affect children and those who are much older. AS is more common in men, but occurs in women as well. Most individuals who have AS also have a gene that produces a “genetic marker”– in this case, a protein– called HLA-B27. This marker is found in over 95% of people in the Caucasian population with AS (the association between ankylosing spondylitis and HLA-B27 varies greatly between ethnic and racial groups. It is important to note, however, that you do not have to be HLA-B27 positive to have AS. Also, a majority of the people with this marker never contract ankylosing spondylitis. Undifferentiated spondyloarthritis has an onset of the disease which is insidious and, even years of disease inflammation or calcification of the sacroiliac joints (the joints where the spine meets the pelvis) is often absent or mild on routine x-rays. According to some experts, the age of onset is very wide and tends to peak at age 50. Unlike AS, USpA is more common in females and only 20-25% of people with USpA are HLA-B27 positive. Some people with undifferentiated spondyloarthropathy later develop symptoms of the other forms of spondylitis, such as AS, but many will continue to have chronic, but not severe symptoms, and remain “undifferentiated.” [http://www.spondylitis.org/about/undif.aspx]

In juvenile spondyloarthritis, sometimes the symptoms are episodic and unpredictable, seeming to come and go without an obvious cause over a long period of time. This cycle of disease flare up followed by remission may be repeated many times. It is important to note that the disease progression and the severity of symptoms vary in each person. Some children may experience a mild, short-term disease, whereas others experience a severe, long-term and disabling condition. The more common symptoms of juvenile spondyloarthritis include arthritic pain, especially around the heels or toes, around the knee and in the lower back. Frequently, the first symptom is pain at the site where ligaments and tendons attach to the bone (the inflammation at this location is called enthesitis). Months or years later, other joints may be affected, particularly joints of the spine or sacroiliac (SI) joints – the joints at the base of the spine, where the spine meets the pelvis. At the beginning of the disease, children often have inflamed, swollen joints like the knees and ankles, but in adults, the spine is more likely to be involved. This inflammation can cause permanent damage if left untreated. Sometimes children with spondyloarthritis develop other symptoms as well. These include fever, psoriasis (a chronic skin rash), other rashes, colitis or Crohn’s disease (inflammation of the intestines), and iritis (inflammation involving the eye). Rare complications may affect the heart, kidneys, or spinal cord. It is also important to know the exact cause is unknown, but genetics do play a key role. Much like in adult-onset spondyloarthropathies, the genetic marker, HLA-B27 is often found in those with JSpa. [http://www.spondylitis.org/about/juvenile.aspx]

About 20% of people who develop Psoriatic Arthritis will eventually have spinal involvement, which is called psoriatic spondylitis. The inflammation in the spine can lead to complete fusion – as in ankylosing spondylitis – or skip areas where, for example, only the lower back and neck are involved. Those with spinal involvement are most likely to test positive for the HLA-B27 genetic marker. The symptoms of psoriasis include scaly red patches appearing anywhere on the body, but often on the scalp, elbows, knees and lower end of the backbone. In psoriatic arthritis, the skin condition is accompanied by arthritis symptoms: the scaly patches on the skin caused by psoriasis; pain and swelling in the fingers or toes, sometimes the swelling causing a “sausage” appearance; small indentations, lifting and /or discoloration of the fingernails or toenails; pain and swelling in the joints; pain and stiffness of the spine, especially after prolonged inactivity; inflammatory eye conditions of the eye such as iritis or conjunctivitis which can cause redness, pain, blurred vision and sensitivity to light. [http://www.spondylitis.org/about/psoriatic.aspx]

Reactive Arthritis usually develops 2-4 weeks after the infection. A tendency exists for more severe and long-term disease in patients who do test positive for HLA-B27 as well as those who have a family history of the disease. Symptoms include: pain, swelling and stiffness in the joints including the knees, ankles and feet; skin rashes that commonly appear as thickened red or brown spots, scaling rashes on the palms of the hands or soles of the feet, or a red scaling rash on the penis; involved fingers and toes that often swell, causing the so-called “sausage digits;” fingernails and toenails which may become thickened and crumble as if infected by fungus; fever and chills; inflammation of the eye (conjunctivitis, uveitis or iritis) that can cause redness, pain, sensitivity to light and skewed vision; enthesopathy – inflammation where the tendon attaches to the bone; inflammation and pain in the lower back or pelvic area; cystitis, which is an inflammation of the bladder or urinary tract, causing frequent urination and a burning sensation when urinating; genital sores appearing on the shaft of the penis or scrotum, or in women, on the external areas of the genitals. These are usually blisters that break open and crust over. Although they heal without scarring, these blisters can be a source of great anxiety in those with ReA. [http://www.spondylitis.org/about/reactive.aspx]


Ankylosing spondylitis and related diseases tend to run in families, so there is a genetic factor involved as well. Those who test positive for the HLA-B27 genetic marker are much more likely to have spinal involvement with enteropathic arthritis than those who test negative. Ulcerative colitis and Crohn’s disease are the two types of IBD most commonly associated with enteropathic arthritis in spondylitis. Abdominal pain and bloody diarrhea are the most common symptoms of IBD. Arthritis symptoms may precede the IBD symptoms. About one in five people with enteropathic arthritis will have inflammatory arthritis in one or more peripheral (limb) joints such as an arm or leg, although the lower limbs are more commonly affected. The severity of the peripheral arthritis normally coincides with the severity of the IBD, thus when diarrhea and abdominal pain are flaring, the peripheral arthritis tends to flare as well. About one in six people with IBD also has spinal inflammation, although this inflammation is independent of the severity of the bowel disease symptoms. In many, this may just be arthritis in the sacroiliac (SI) joints, but in about five percent of people, the entire spine is involved, as it is in AS.[http://www.spondylitis.org/about/ibd.aspx]



When I was writing this, I kept thinking that I should have a site like Google just for symptoms. It would be like an online search tool for symptoms only, but it wold only be for symptoms~kind of like Web MD’s search tool. The part that would be most interesting is that it would come from me since I’ve actually experienced most of the symptoms myself. It would be like asking me personally~have you had this symptom Dana Morningstar? How did it feel? What did the doctors tell you? What did you do about it? Could you give me some advice? It would be so cool?….Someday in the future I hope…
 Image taken from pharmamkting.blogspot.com
Image taken from pharmamkting.blogspot.com